A hysterectomy is the surgical removal of the uterus. Different portions of the uterus, as well as other organs, may be removed at the same time.
The types of hysterectomy include:
-
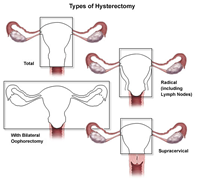
Total hysterectomy. Includes the removal of the entire uterus, including the fundus (the part of the uterus above the openings of the fallopian tubes) and the cervix, but not the tubes or ovaries. This is the most common type of hysterectomy.
-
Hysterectomy with salpingo-oophorectomy. Includes the removal of one or both ovaries, and the fallopian tubes, along with the uterus.
-
Radical hysterectomy. Includes the removal of the uterus, cervix, the top portion of the vagina, most of the tissue that surrounds the cervix in the pelvic cavity, and may include the removal of the pelvic lymph nodes. This is done in some cases of cancer.
-
Supracervical hysterectomy (partial or subtotal hysterectomy). Removal of the body of the uterus while leaving the cervix intact
In addition to the different types of hysterectomies, there are different surgical techniques used to perform a hysterectomy. Surgical hysterectomy techniques include:
-
Abdominal hysterectomy. The uterus is removed through the abdomen via a surgical incision about six to eight inches long. This procedure is most commonly used when the ovaries and fallopian tubes are being removed, when the uterus is enlarged, or when disease has spread to the pelvic cavity, as in endometriosis or cancer. The main surgical incision can be made either vertically, from the navel down to the pubic bone, or horizontally, along the top of the pubic hairline.
-
Vaginal hysterectomy. The uterus is removed through the vaginal opening. This procedure is most often used in cases of uterine prolapse, or when vaginal repairs are necessary for related conditions. No external incision is made, which means there is no visible scarring.
-
Laparoscope-assisted vaginal hysterectomy/robot-assisted laparoscopic hysterectomy. Vaginal hysterectomy is performed with the aid of a laparoscope, a thin, flexible tube containing a video camera. Thin tubes are inserted through tiny incisions in the abdomen near the navel. The uterus is then removed in sections through the laparoscope tube or through the vagina. In a robot-assisted laparoscopic hysterectomy, the doctor inserts the laparoscope and other instruments, then uses a computer station to control the instruments.
The type of hysterectomy performed and the technique used to perform the procedure will be determined by your doctor, based on your particular situation.
For women who have not yet reached menopause, having a hysterectomy means that menstruation will no longer occur, nor will pregnancy be possible.
Reasons for performing a hysterectomy include, but are not limited to, the following:
-
Fibroid tumors. Nonmalignant tumors.
-
Endometriosis. A condition in which endometrial cells grow outside of the uterus, attaching themselves to other organs in the pelvic cavity, resulting in chronic pelvic pain, pain during sex, and prolonged or heavy bleeding.
-
Abnormal uterine bleeding. This is often due to endometrial hyperplasia, an over thickening of the uterine lining that may cause abnormal bleeding.
-
Cancer. Cervical, ovarian, or endometrial cancer is the diagnosis in approximately 10 percent of hysterectomies.
-
Blockage of the bladder or intestines by the uterus or a growth
Hysterectomy may also be performed when uterine prolapse (the uterus drops down into the vagina) occurs, or in the presence of chronic pelvic conditions, such as pelvic pain or pelvic inflammatory disease, that do not respond to other treatments.
There may be other reasons for your doctor to recommend a hysterectomy.
As with any surgical procedure, complications may occur. Some possible complications include, but are not limited to, the following:
-
Hemorrhage
-
Injury to the ureters (tubes that carry urine from the kidneys to the bladder) and urinary bladder
-
Infection
-
Injury to the bowel or other intestinal organs
-
Difficulty with urination or urinary incontinence
Women who have not reached menopause prior to a hysterectomy may experience menopausal symptoms such as hot flashes, mood swings, and vaginal dryness after the procedure if the ovaries are removed. Women will no longer have menstrual periods after a hysterectomy.
Mood swings, depression, and feelings of loss of sexual identity may occur after hysterectomy.
There may be other risks depending on your specific medical condition. Be sure to discuss any concerns with your doctor prior to the procedure.
In the hospital
After the procedure, you will be taken to the recovery room for observation. Your recovery process will vary depending on the type of procedure performed and the type of anesthesia that is given. Once your blood pressure, pulse, and breathing are stable and you are alert, you will be taken to your hospital room.
Abdominal cramping may occur after the surgery. You may receive pain medication as needed, either by a nurse or by administering it yourself through a device connected to your intravenous line.
If your procedure was an abdominal hysterectomy, you may have a thin, plastic tube inserted through your nose into your stomach to remove air that you swallow. The tube will be removed when your bowels resume normal function. You will not be able to eat or drink until the tube is removed.
You may have small to moderate amounts of vaginal drainage for several days. The nurse will check the sanitary pads periodically to monitor the amount of drainage.
You will be encouraged to get out of bed within a few hours after a vaginal procedure or by the next day after an abdominal procedure. In addition, you should perform coughing and deep breathing exercises as instructed by your nurse.
Depending on your situation, you may be given liquids to drink a few hours after surgery. Your diet may be gradually advanced to more solid foods as tolerated.
Arrangements will be made for a follow-up visit with your doctor, usually several weeks after the procedure.
At home
Once you are home, it is important to keep the incision clean and dry. Your doctor will give you specific bathing instructions. If stitches or surgical staples are used, they will be removed during a follow-up office visit, if they were not removed prior to your discharge from the hospital. If adhesive strips are used, they should be kept dry and generally will fall off within a few days.
The incision and the abdominal muscles may ache, especially after long periods of standing. If a laparoscope was used, you may experience shoulder pain from the carbon dioxide in your abdomen. Take a pain reliever for soreness as recommended by your doctor. Aspirin or certain other pain medications may increase the chance of bleeding. Be sure to take only recommended medications.
Walking and limited movement are generally encouraged, but strenuous activity should be avoided. Your doctor will instruct you about when you can return to work and resume normal activities.
Avoid becoming constipated by including fiber and plenty of liquids in your diet. Your doctor may recommend a mild laxative.
If a laparoscopic procedure was performed, you should avoid drinking carbonated beverages for one to two days after the procedure. This will help minimize the discomfort associated with the carbon dioxide gas. In addition, drinking carbonated beverages may cause nausea.
You should not use a douche, tampons, engage in sexual intercourse, or return to work until your doctor advises you to do so.
Notify your doctor to report any of the following:
-
Fever and/or chills
-
Redness, swelling, or bleeding or other drainage from the incision site(s)
-
Increased pain around the incision site(s)
-
Abdominal pain, cramping, or swelling
-
Increased vaginal bleeding or other drainage
-
Leg pain
Following a hysterectomy, your doctor may give you additional or alternate instructions, depending on your particular situation.